Introduction
Hypertension is one of the most common worldwide diseases afflicting humans. Because of the associated morbidity and mortality and the cost to the society, hypertension is an important public health challenge. Over the past several decades, extensive research, widespread patient education, and a concerted effort on the part of health care professionals had lead to decreased mortality and morbidity rates from the multiple organ damage arising from years of untreated hypertension.
Hypertension is the most important modifiable risk factor for coronary heart disease, stroke, congestive heart failure, and end-stage renal diseases, and peripheral vascular disease. Therefore, health care professionals must not only indentify and treat patient with hypertension but also promote healthy lifestyle and preventive strategies to decrease the prevalence of hypertension in the general population.

Definition and Classification of Hypertension
The classification of high BP, although arbitrary, is useful as clinicians must make treatment decisions based on the measured BP and the patients’ associated cardiovascular/cerebrovascular risks and comorbidities. Table 1 provides a classification of BP for adults (age 18 and older). The WHO-ISH guidelines in principle have adopted a similar classification. These criteria are for subjects who are not on any antihypertensive medication and who are not acutely ill.
Table 1. Classification of blood pressure for adults age 18 and older.
Category | Systolic (mmHg) | Diastolic (mmHg) | Prevalence in Malaysia (%) |
Optimum | < 120 | <80 | 32 |
Prehypertension | 120-139 | 80-89 | 37 |
Hypertension | |||
Stage 1 | 140-159 | 90-99 | 20 |
Stage 2 | 160-179 | 100-109 | 8 |
Stage 3 | >180 | >110 | 4 |
Epidemiology of Hypertension in Malaysia
According to cross sectional study “Prevalence, awareness, treatment and control of hypertension in Malaysia: A national study of 16,440 subjects.” Rampal L, Rampal S, Azhar MZ, Rahman AR. (Public Health. 2008 Jan;122(1):11-8. Epub 2007 Nov 5.); the overall prevalence of hypertension for subjects aged 15 years was 27.8%. The prevalence of hypertension was significantly higher in males (29.6%) compared with females (26.0). Only 34.6% of the subjects with hypertension were aware of their hypertensive status, and 32.4% were taking antihypertensive medication. Amongst the latter group, only 26.8% had their blood pressure under control. The prevalence of hypertension amongst those aged 30 years has increased from 32.9% in 1996 to 40.5% in 2004.
Risk Factors

-Family history
-Excessive alcohol intake
-High salt intake
-Low potassium intake
-Age
-Stress
-Smoking
-Obesity
-Atherosclerosis
Pathophysiology
Arterial blood pressure is a product of cardiac output and systemic vascular resistance. Therefore, determinants of blood pressure include factors that affect cardiac output and arteriolar vascular physiology. Blood viscosity, vascular wall sheer conditions (rate and stress), and blood flow velocity (mean and pulsatile components) have potential relevance with regard to the regulation of blood pressure in humans by vascular and endothelial function. Furthermore, changes in vascular wall thickness affect the amplification of peripheral vascular resistance in hypertensive patients and result in reflection of waves back to the aorta, increasing systolic blood pressure. Circulating blood volume is regulated by renal salt and water handling, a phenomenon that plays a particularly important role in salt-sensitive hypertension.
Regulation of blood pressure
Regulation of blood pressure
Regulation of normal blood pressure is a complex process. Although a function of cardiac output and peripheral vascular resistance, both of these variables are influenced by multiple factors.
The factors affecting cardiac output include sodium intake, renal function, and mineralocorticoids; the inotropic effects occur via extracellular fluid volume augmentation and an increase in heart rate and contractility. Peripheral vascular resistance is dependent upon the sympathetic nervous system, humoral factors, and local autoregulation. The sympathetic nervous system produces its effects via the vasoconstrictor alpha effect or the vasodilator beta effect. The humoral actions on peripheral resistance are also mediated by other mediators such as vasoconstrictors (angiotensin and catecholamines) or vasodilators (prostaglandins and kinins).
Autoregulation of blood pressure occurs by way of intravascular volume contraction and expansion regulated by the kidney, as well as via transfer of transcapillary fluid. Through the mechanism of pressure natriuresis, salt and water balance is achieved at heightened systemic pressure, as proposed by Guyton. Interactions between cardiac output and peripheral resistance are autoregulated to maintain a set blood pressure in an individual. For example, constriction of the arterioles elevates arterial pressure by increasing total peripheral resistance, whereas venular constriction leads to redistribution of the peripheral intravascular volume to the central circulation, thereby increasing preload and cardiac output.
Pathogenesis of hypertension & Causes

Essential Hypertension
The pathogenesis of essential hypertension is multifactorial and highly complex. Multiple factors modulate the blood pressure for adequate tissue perfusion and include humoral mediators, vascular reactivity, circulating blood volume, vascular caliber, blood viscosity, cardiac output, blood vessel elasticity, and neural stimulation. A possible pathogenesis of essential hypertension has been proposed in which multiple factors, including genetic predisposition, excess dietary salt intake, and adrenergic tone, may interact to produce hypertension. Although genetics appears to contribute to essential hypertension, the exact mechanism has not been established.
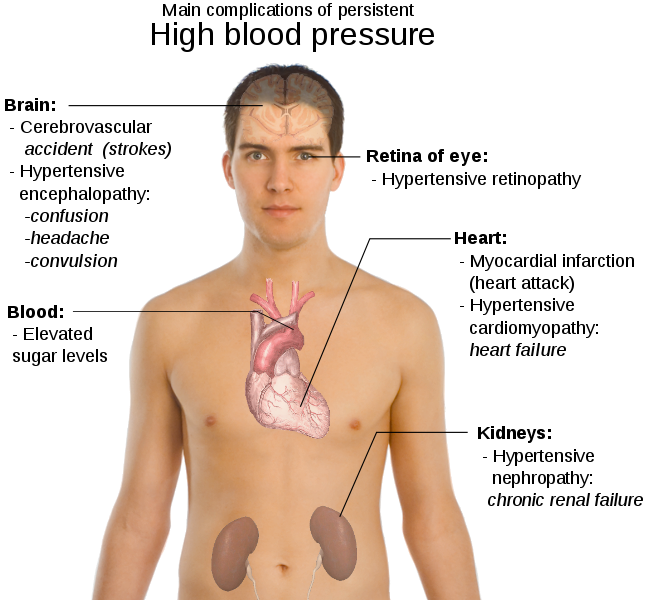
The natural history of essential hypertension evolves from occasional to established hypertension. After a long invariable asymptomatic period, persistent hypertension develops into complicated hypertension, in which target organ damage to the aorta and small arteries, heart, kidneys, retina, and central nervous system is evident. The progression begins with prehypertension in persons aged 10-30 years (by increased cardiac output) to early hypertension in persons aged 20-40 years (in which increased peripheral resistance is prominent) to established hypertension in persons aged 30-50 years, and, finally, to complicated hypertension in persons aged 40-60 years.
One mechanism of hypertension has been described as high-output hypertension. High-output hypertension results from decreased peripheral vascular resistance and concomitant cardiac stimulation by adrenergic hyperactivity and altered calcium homeostasis. A second mechanism manifests with normal or reduced cardiac output and elevated systemic vascular resistance due to increased vasoreactivity. Another (and overlapping) mechanism is increased salt and water reabsorption (salt sensitivity) by the kidney, which increases circulating blood volume.
The vasoreactivity of the vascular bed, an important phenomenon mediating changes of hypertension, is influenced by the activity of vasoactive factors, reactivity of the smooth muscle cells, and structural changes in the vessel wall and vessel caliber, expressed by a lumen-to-wall ratio. Patients who develop hypertension are known to develop a systemic hypertensive response secondary to vasoconstrictive stimuli. Alterations in structural and physical properties of resistance arteries, as well as changes in endothelial function, are probably responsible for this abnormal behavior of vasculature. Furthermore, vascular remodeling occurs over the years as hypertension evolves, thereby maintaining increased vascular resistance irrespective of the initial hemodynamic pattern.
The vasoreactivity of the vascular bed, an important phenomenon mediating changes of hypertension, is influenced by the activity of vasoactive factors, reactivity of the smooth muscle cells, and structural changes in the vessel wall and vessel caliber, expressed by a lumen-to-wall ratio. Patients who develop hypertension are known to develop a systemic hypertensive response secondary to vasoconstrictive stimuli. Alterations in structural and physical properties of resistance arteries, as well as changes in endothelial function, are probably responsible for this abnormal behavior of vasculature. Furthermore, vascular remodeling occurs over the years as hypertension evolves, thereby maintaining increased vascular resistance irrespective of the initial hemodynamic pattern.
Secondary Hypertension
Secondary hypertension is the hypertension arises due to the complication of other systemic disease mainly divided into four major categories which are renal disease, endocrine disease, cardiovascular disease and neurological disease.
Renal Disease
-Acute glomerulonephritis
-Chronic renal disease
-Polycyctic kidney disease
-Renal artery stenosis
Renal artery fibromuscular dysplasia
Renal vasculitis
Renin-producing tumor
Endocrine Disease
-Adrenal hyperfunction
-Cushing syndrome
-Primary aldosteronism
-Congenital adrenal hyperplasia
-Licorice ingestion
-Exogenous hormones
-Glucocortocoids
-Oestrogen
-Sympathomimetics
-Tyramine Contaning food
-Monoamine inhibitors
-Phaeochromocytoma
-Acromegaly
-Hyperthyroidism
-Hypothyroidism
Cardiovascular
-Coarctation of aorta
-Polyarteritis nodosa
-Increased intravascular volume
-Increased cardiac output
-Rigidity of Aorta
Neurology
-Psychogenic
-Increased intracranial pressure
-Sleep apnoea
Malignant Hypertension
The pathogenesis of malignant hypertension is not fully understood. It is being characterised by severe hypertension with systolic > 200mmHg and diastolic >130mmHg with renal failure, retinal haemorrhage with exudates with/out papilloedema. It is a rare (5% of hypertensive patient) but very serious form of high blood pressure and is a medical emergency. All the organ systems are at risk from malignant hypertension, but eyes, kidney and brain seem to at greatest risk. The characteristic vascular lesion is fibrinoid necrosis of arterioles and small arteries, which causes the clinical manifestations of end-organ damage. Red blood cells are damaged as they flow through vessels obstructed by fibrin deposition, resulting in microangiopathic hemolytic anemia.

Onion skin, concentric, laminated thickening of wall of arterioles with progressing narrowing of lumina. The changes are accompanied by deposits of fibrinoid necrosis of vessel wall referred as necrotizing arteriolitis in kidney.
SIGNS AND SIYMPTOMS OF HYPERTENSION
Most people with hypertension don't have any symptoms. This is because hypertension doesn't cause problems over a day or weeks or even months. It usually takes several years for hypertension to cause noticeable symptoms, and even when it does cause problems, the symptoms are often mild and nonspecific meaning they could be caused by several different conditions. As a result, hypertension is often referred to as "the silent killer." People with hypertension typically don't even realize they have it until they have blood pressure readings that are too high. Sometimes people with markedly elevated blood pressure may develop:
1. Chronic headaches. Chronic headaches usually last for days (rather than hours). Most people have experienced headaches from time to time
2. Dizziness or Vertigo
3. Blurry or double vision.
4. Drowsiness
5. Nausea
6. Shortness of breath. Usually when this occurs people start to get a little concerned. Often by this time though the blood pressure has probably reached high enough levels to be dangerous.
7. Heart palpitations
8. Fatigue - general tiredness
9. A flushed face
10. Nosebleeds
11. A strong need to urinate often (especially during the night)
12. Tinnitus (ringing in the ear). Many people have tinnitus for years and have no real serious underlying problem.
Physical Examination
An accurate measurement of blood pressure is the key to diagnosis. Several determinations should be made over a period of several weeks.
At any given visit, an average of 3 blood pressure readings taken 2 minutes apart using a mercury manometer is preferable. Blood pressure should be measured in both the supine and sitting positions, auscultating with the bell of the stethoscope. On the first visit, blood pressure should be checked in both arms and in one leg to avoid missing the diagnosis of coarctation of aorta or subclavian artery stenosis.
As the improper cuff size may influence blood pressure measurement, a wider cuff is preferable, particularly if the patient's arm circumference exceeds 30 cm.
The patient should rest quietly for at least 5 minutes before the measurement.

"Non-dipping" is the loss of the usual physiologic nocturnal drop in blood pressure and is associated with an increased cardiovascular risk.
A funduscopic evaluation of the eyes should be performed to detect any evidence of hypertensive retinopathy. These are flame-shaped haemorrhages and cotton wool exudates.
A funduscopic evaluation of the eyes should be performed to detect any evidence of hypertensive retinopathy. These are flame-shaped haemorrhages and cotton wool exudates.
Palpation of all peripheral pulses should be performed. Absence of femoral pulses suggests coarctation of the aorta or severe peripheral vascular disease.
Look for renal artery bruit over the upper abdomen; the presence of a unilateral bruit with both a systolic and diastolic component suggests renal artery stenosis.
Diagnostic Examination
Laboratory Studies
- Unless a secondary cause for hypertension is suspected, only the following routine laboratory studies should be performed:
- CBC count, serum electrolytes, serum creatinine, serum glucose, uric acid, and urinalysis
- Lipid profile (total cholesterol, low-density lipoprotein [LDL], high-density lipoprotein [HDL], and triglycerides)
- Additional tests described below are indicated when specific clinical situations warrant further investigation.
- Microalbuminuria is an early indication of diabetic nephropathy and is also a marker for a higher risk of cardiovascular morbidity and mortality. Present recommendations suggest that individuals with type I diabetes should be screened for microalbuminuria. Usefulness of this screening in hypertensive patients without diabetes has not been established.
- Measurement of the aldosterone /plasma renin activity ratio is performed to detect evidence of primary hyperaldosteronism. A ratio of more than 20-30 is suggestive of this condition. Hypokalemia and metabolic alkalosis are relatively late manifestations of this disorder. A 24-hour urinary excretion of aldosterone under salt-loading conditions confirms the diagnosis.
- Determination of a sensitive thyroid-stimulating hormone (TSH) level excludes hypothyroidism or hyperthyroidism as a cause of hypertension.
- If pheochromocytoma is suspected, urinary catecholamines and fractionated metanephrines are the tests of choice. Plasma fractionated metanephrines have specificity, but their sensitivity is too low for screening purposes. Urinary vanillylmandelic acid (VMA) is no longer recommended because of its poor sensitivity and specificity.
Imaging Studies
- Echocardiography: The limited echocardiography study, rather than the complete examination, may detect LVH more frequently than electrocardiography. The main indication for limited echocardiography is evaluation for end organ damage in a patient with borderline high blood pressure. Therefore, the presence of LVH despite normal or borderline high blood pressure measurements requires antihypertensive therapy.
- Imaging studies for renovascular stenosis: If the patient's history suggests renal artery stenosis and if a corrective procedure is considered, further radiologic investigations are performed, such as computed tomography (CT) angiography and magnetic resonance angiography (MRA). Concern over the risk of nephrogenic systemic fibrosis due to gadolinium has reduced the use of MRA, particularly in patients with chronic kidney disease who have a GFR of less than 30 mL/min. This is a rare debilitating, life threatening disorder associated with gadolinium. CT angiography carries the risk of dye nephropathy, particularly in persons with diabetes who have chronic kidney disease.
- Digital subtraction angiography with arterial injection of radiocontrast dye: This technique is the gold standard, but it carries the risk of dye nephropathy and atheroemboli in patients with diabetes or chronic kidney disease.
Other Tests
- Routine testing includes electrocardiograms.
- Ambulatory blood pressure monitoring: Indications for ambulatory blood pressure monitoring include labile blood pressure, a discrepancy between blood pressure measurement inside and outside the physician's office, and poor blood pressure control. Ambulatory monitoring also identifies patients who have the distinct syndrome called white coat hypertension.
Management

In patients with newly diagnosed uncomplicated hypertension and no compelling indications, choice of first line monotherapy includes angiotensin-converting enzyme inhibitors (ACEI), angiotensin receptor blockers (ARB), calcium channel blockers (CCB) and diuretics. Beta-blockers are no longer recommended for first line monotherapy in this group of patients. However, beta-blockers may be considered in younger people, particularly:
• Those with an intolerance or contraindication to ACEIs and ARBs or
• Women of child-bearing potential or
• Patients with evidence of increased sympathetic drive
In patients with stage 1 hypertension, treatment should be started with a single drug at low dose. Monotherapy can lower BP to <140/90 mmHg in approximately 40 – 60% of patients with mild to moderate hypertension. If after a sufficient period of treatment (up to six weeks) with monotherapy BP is still not controlled, three options are available
• The dose of the initial drug can be increased
• The drug can be substituted with another class of drug
• A second drug can be added
Increasing the dose of the initial antihypertensive agent or adding a second agent is preferred if the patient shows response to the initial drug but target BP is not achieved. The former, however, may give rise to dose-related adverse effects. Properly selected antihypertensive combinations may also mitigate the adverse effects of each other. To improve compliance, a fixed-dose combination drug may be considered. If the patient does not show response or does not tolerate the initial drug, drug substitution is recommended.



Non-Pharmacological Prevention in 6 Simple Steps
Step 1: Following a Healthy Eating Pattern
Research has shown that following a healthy eating plan can both reduce the risk of developing high blood pressure and lower an already elevated blood pressure.
Step 2: Reducing Salt and Sodium in Your Diet
A key to healthy eating is choosing foods lower in salt and sodium. The current recommendation is to consume less than 2.4 grams (2,400 milligrams [mg] ) of sodium a day. That equals 6 grams (about 1 teaspoon) of table salt a day. The 6 grams include ALL salt and sodium consumed, including that used in cooking and at the table. For someone with high blood pressure, the doctor may advise eating less salt and sodium, as recent research has shown that people consuming diets of 1,500 mg of sodium had even better blood pressure lowering benefits. These lower-sodium diets also can keep blood pressure from rising and help blood pressure medicines to work better.
Step 3: Maintaining a Healthy Weight
Being overweight increases your risk of developing high blood pressure. In fact, blood pressure rises as body weight increases. Losing even 10 pounds can lower blood pressure — and it has the greatest effect for those who are overweight and already have hypertension.
Step 4: Being Physically Active
Being physically active is one of the most important steps you can take to prevent or control high blood pressure. It also helps reduce your risk of heart disease. It doesn't take a lot of effort to become physically active.
Step 5: Limiting Alcohol Intake
Drinking too much alcohol can raise blood pressure. It also can harm the liver, brain, and heart. Alcoholic drinks also contain calories, which matter if you are trying to lose weight. If you drink alcoholic beverages, have only a moderate amount — one drink a day for women; two drinks a day for men.
Step 6: Quitting Smoking
Smoking injures blood vessel walls and speeds up the process of hardening of the arteries. This applies even to filtered cigarettes. So even though it does not cause high blood pressure, smoking is bad for anyone, especially those with high blood pressure. If you smoke, quit. If you don't smoke, don't start. Once you quit, your risk of having a heart attack is reduced after the first year. So you have a lot to gain by quitting.
Step 2: Reducing Salt and Sodium in Your Diet
A key to healthy eating is choosing foods lower in salt and sodium. The current recommendation is to consume less than 2.4 grams (2,400 milligrams [mg] ) of sodium a day. That equals 6 grams (about 1 teaspoon) of table salt a day. The 6 grams include ALL salt and sodium consumed, including that used in cooking and at the table. For someone with high blood pressure, the doctor may advise eating less salt and sodium, as recent research has shown that people consuming diets of 1,500 mg of sodium had even better blood pressure lowering benefits. These lower-sodium diets also can keep blood pressure from rising and help blood pressure medicines to work better.
Step 3: Maintaining a Healthy Weight
Being overweight increases your risk of developing high blood pressure. In fact, blood pressure rises as body weight increases. Losing even 10 pounds can lower blood pressure — and it has the greatest effect for those who are overweight and already have hypertension.
Step 4: Being Physically Active
Being physically active is one of the most important steps you can take to prevent or control high blood pressure. It also helps reduce your risk of heart disease. It doesn't take a lot of effort to become physically active.
Step 5: Limiting Alcohol Intake
Drinking too much alcohol can raise blood pressure. It also can harm the liver, brain, and heart. Alcoholic drinks also contain calories, which matter if you are trying to lose weight. If you drink alcoholic beverages, have only a moderate amount — one drink a day for women; two drinks a day for men.
Step 6: Quitting Smoking
Smoking injures blood vessel walls and speeds up the process of hardening of the arteries. This applies even to filtered cigarettes. So even though it does not cause high blood pressure, smoking is bad for anyone, especially those with high blood pressure. If you smoke, quit. If you don't smoke, don't start. Once you quit, your risk of having a heart attack is reduced after the first year. So you have a lot to gain by quitting.
Neurology
- Intracerebral hemorrhage
-Lacunar infarcts
-Encephalopathy
-Thrombotic stroke
-Transient ischemic attack
Ophthalmology
-Fundal haemorrhages
-Exudates
-Papilloedema
Cardiovascular System
- Left ventricular hypertrophy
-Congestive heart failure
-Angina pectoris
-Myocardial infarction
-Aortic dissection
-Diffuse arthrosclerosis
-Aneurysm
Nephrology
-Nephrosclerosis
-Nephrosclerosis
-Renal artery stenosis
-Renal failure
Prognosis
Prognosis of hypertension depends on how severe the condition is and how long a person has had it. It is affected by other conditions such as Diabetes Mellitus. Most of the time it can be controlled by lifestyle changes, medication or a combination of both. But a large percentage of people with hypertension are unaware that they have it.
Untreated high blood pressure increases a person’s risk of developing heart disease such as heart failure, heart attack or sudden cardiac death, kidney failure or stroke at an early age. High blood pressure is the most important risk factor for stroke. It is also one of the three most important risk factors for heart attack that a person can modify. Treatments that lower blood pressure decreases risk for stroke and heart failure. Without treatment less than 5% of people with malignancy hypertension survive for years.
Untreated high blood pressure increases a person’s risk of developing heart disease such as heart failure, heart attack or sudden cardiac death, kidney failure or stroke at an early age. High blood pressure is the most important risk factor for stroke. It is also one of the three most important risk factors for heart attack that a person can modify. Treatments that lower blood pressure decreases risk for stroke and heart failure. Without treatment less than 5% of people with malignancy hypertension survive for years.
Live Testimony: I am greatful to Dr Itua ,the powerful herbal healer that rescued me from HIV/AIDS and HERPES. I was diagnosed of these disease since 2012 and because of this, i was very unhappy with my life and i went into research on how i can get cured and i saw a testimony of a lady on how she was cured from HERPES by Dr Itua , i decided to give him a try and when i contact him, he assure me that he will help me and send me the cure and i believed in him because all i wanted was to be cured, so he prepared a herbal cure for me and send it to me through DHL and gave me instructions on how to use it and after one week i should go to hospital for checkup and after one week of using the herbal medicine, i went to the hospital for test and to my surprise the test stated that i am HIV/AIDS with HERPES negative and i am fully cured from the diseases. This gladdens my heart and everybody in the hospital was surprised even the Medical Doctor, So viewers Dr Itua is a God Gifted man and he can cure so many diseases like HIV/AIDS, HERPES,CANCER of all kind, PILE, KIDNEY PROBLEM, SYPHILIS, DIABETICS and lot's more. You can contact him through his email:drituaherbalcenter@gmail.com or call and whatsapp him on +2348149277967 . I will continue to share this great testimony on the internet and all over the world for the good job Dr has done for me.///
ReplyDelete